What is Cervical cancer
Cervical cancer is cancer that's found anywhere in the cervix, which is the opening between the vagina and the womb.
common in women aged between 30 and 35, but it can happen at any age.
Signs and Symptoms of Cervical Cancer
Women with early cervical cancers and pre-cancers usually have no symptoms. Symptoms often do not begin until the cancer becomes larger and grows into nearby tissue. When this happens, the most common cervical cancer symptoms are:
Abnormal vaginal bleeding, such as bleeding after vaginal sex, bleeding after menopause, bleeding and spotting between periods, or having (menstrual) periods that are longer or heavier than usual. Bleeding after douching may also occur.
An unusual discharge from the vagina − the discharge may contain some blood and may occur between your periods or after menopause.
Pain during sex.
Pain in the pelvic region.
Signs and symptoms of cervical cancer seen with more advanced disease can include:
Swelling of the legs.
Problems urinating or having a bowel movement.
Blood in the urine.
These signs and symptoms can also be caused by conditions other than cervical cancer. Still, if you have any of these cervical cancersymptoms, see a health care professional right away. Ignoring symptoms may allow the cancer to grow to a more advanced stage and lower your chance for successful treatment.
For the best chances for treatment to be successful, don't wait for symptoms and signs of cervical cancer to appear. Have regular screening tests for cervical cancer.
Tests for Cervical Cancer
Finding cervical cancer often starts with an abnormal HPV (human papillomavirus) or Pap test result. This will lead to further tests which can diagnose cervical cancer or pre-cancer. The Pap test and HPV test are screening tests, not diagnostic tests. They cannot tell for certain if you have cervical cancer. An abnormal Pap test or HPV test result may mean more testing is needed to see if a cancer or a pre-cancer is present.
Cervical cancer may also be suspected if you have symptoms like abnormal vaginal bleeding or pain during sex. Your primary doctor or gynecologist often can do the tests needed to diagnose pre-cancers and cancers. If you are diagnosed with invasive cancer, your doctor will probably refer you to a gynecologic oncologist, a doctor who specializes in cancers of women's reproductive systems.
Tests for people with symptoms of cervical cancer or abnormal cervical screening test results
Medical history and physical exam
First, the doctor will ask you about your personal and family medical history. This includes information related to risk factors and symptoms of cervical cancer. A complete physical exam will help evaluate your general state of health. You will have a pelvic exam and maybe a Pap test if one has not already been done. In addition, your lymph nodes will be felt to see if the cancer has spread (metastasis).
Understanding abnormal cervical screening test results
Your current screening test results along with your past test results, determine your risk of developing cervical cancer. Your doctor will use them to figure out your next test or treatment. It could be a follow-up screening test in a year, a colposcopy, or one of the other procedures discussed below to treat any pre-cancers that might be found.
Because there are many different follow-up or treatment options depending on your specific risk of developing cervical cancer, it is best to talk to your health care provider about your screening results in more detail, to fully understand your cervical cancer risk and the best follow-up plan for you.
Endocervical curettage (endocervical scraping)
If colposcopy does not show any abnormal areas or if the transformation zone (the area at risk for HPV infection and pre-cancer) cannot be seen with the colposcope, another method must be used to check that area for cancer.
A narrow instrument (either a curette or a brush) is inserted into the endocervical canal (the part of the cervix closest to the uterus). The curette or brush is used to scrape the inside of the canal to remove some of the tissue, which is then sent to the lab to be checked. During or after this procedure, patients may feel a cramping pain, and they may also have some light bleeding.
Colposcopy
If you have certain symptoms that could mean cancer, if your Pap test result shows abnormal cells, or if your HPV test is positive, you will most likely need to have a procedure called a colposcopy. You will lie on the exam table as you do with a pelvic exam. The doctor will put a speculum in the vagina to help keep it open while examining the cervix with a colposcope. The colposcope is an instrument that stays outside the body and has magnifying lenses. It lets the doctor clearly see the surface of the cervix up close. Colposcopy itself is usually no more uncomfortable than any other speculum exam. It can be done safely even if you are pregnant. Like the Pap test, it is better not to do it during your menstrual period.
The doctor will put a weak solution of acetic acid (similar to vinegar) on your cervix to make any abnormal areas easier to see. If an abnormal area is seen, a small piece of tissue will be removed (biopsy) and sent to a lab to be looked at carefully. A biopsy is the best way to tell for certain if an abnormal area is a pre-cancer, an invasivecancer, or neither.
Cone biopsy
In this procedure, also known as conization, the doctor removes a cone-shaped piece of tissue from the cervix. The base of the cone is formed by the exocervix (outer part of the cervix), and the point or apex of the cone is from the endocervical canal. The tissue removed in the cone includes the transformation zone (the border between the exocervix and endocervix, where cervical pre-cancers and cancers are most likely to start). A cone biopsy can also be used as a treatment to completely remove many pre-cancers and some very early cancers.
The methods commonly used for cone biopsies are the loop electrosurgical excision procedure (LEEP), also called the large loop excision of the transformation zone (LLETZ), and the cold knife cone biopsy.
Loop electrosurgical procedure (LEEP, LLETZ):
In this method, the tissue is removed with a thin wire loop that is heated by electricity and acts as a small knife. A local anesthetic is used for this procedure, and it can be done in your doctor's office.
Cold knife cone biopsy:
This is done in a hospital. A surgical scalpel or a laser is used to remove the tissue instead of a heated wire. You will receive anesthesia during the operation (either a general anesthesia, where you are asleep, or a spinal or epidural anesthesia, where an injection into the area around the spinal cord makes you numb below the waist).
Possible complications of cone biopsies include bleeding, infection and narrowing of the cervix.
Having had any type of cone biopsy will not prevent most women from getting pregnant, but if a large amount of tissue has been removed, women may have a higher risk of giving birth prematurely.
Other tests when cervical cancer is diagnosed
If a biopsy shows that cancer cells are present, your doctor may order certain tests to see if and how far the cancer has spread. Many of the tests described below are not necessary for every patient. Decisions about using these tests are based on the results of the physical exam and biopsy.
Cystoscopy, proctoscopy, and examination under anesthesia
These are most often done when the tumors are large. They are not necessary if the cancer is caught early.
In a cystoscopy, a slender tube with a lens and a light is placed into the bladder through the urethra. This lets the doctor check your bladder and urethra to see if cancer is growing into these areas. Biopsy samples can be removed during cystoscopy for testing in the lab. Cystoscopy can be done under a local anesthetic, but some patients may need general anesthesia. Your doctor will let you know what to expect before and after the procedure.
Proctoscopy is a visual inspection of the rectum through a lighted tube to look for spread of cervical cancer into your rectum.
Your doctor may also do a pelvic exam while you are under anesthesia to find out if the cancer has spread beyond the cervix.
Imaging studies
If your doctor finds that you have cervical cancer, certain imaging studies may be done. These tests can show if and where the cancer has spread, which will help you and your doctor decide on a treatment plan.
Chest x-ray:
Your chest may be x-rayed to see if cancer has spread to your lungs.
Computed tomography (CT):
CT scans are usually done if the tumor is larger or if there is concern about cancer spread. For more information, see CT Scan for Cancer.
Magnetic resonance imaging (MRI):
MRI scans look at the soft tissue parts of the body sometimes better than other imaging tests, like a CT scan. Your doctor will decide which imaging test is best to use in your situation. For more information, see MRI for Cancer.
Positron emission tomography/ computed tomography (PET/CT) scan:
For a PET scan, a slightly radioactive form of sugar (known as FDG) is injected into the blood and collects mainly in cancer cells. Often a PET scan is combined with a CT scan using a special machine that can do both at the same time. This lets the doctor compare areas of higher radioactivity on the PET scan with a more detailed picture on the CT scan. This is the type of PET scan most often used in patients with cervical cancer. This test can help see if the cancer has spread to lymph nodes. PET scans can also be useful if your doctor thinks the cancer has spread but doesn’t know where.
Intravenous urography:
Intravenous urography (also known as intravenous pyelogram, or IVP) is an x-ray of the urinary system taken after a special dye is injected into a vein. This test can find abnormal areas in the urinary tract, caused by the spread of cervical cancer. The most common finding is that the cancer has blocked the ureters (tubes that connect the kidneys to the bladder). IVP is rarely used for patients with cervical cancer because CT and MRI are also good at finding abnormal areas in the urinary tract, as well as others not seen with an IVP.
Cervical Cancer: Stages
What does stage of cancer mean?
The stage of a cancer is how much cancer there is and how far it has spread in your body. Your healthcare provider uses exams and imaging scans to find out the size of the cancer and where it is. Scans can also show if the cancer has grown into nearby areas, and if it has spread to other parts of your body. The stage of a cancer is one of the most important things to know when deciding how to treat the cancer.
Staging can help healthcare providers have an idea about how the cancer may grow, and how certain kinds of treatment may work. Staging can also help give your healthcare team an idea of what kind of outcomes you can expect (prognosis).
What are the stages of cervical cancer?
The staging system most often used for cervical cancer is from the International Federation of Gynecology and Obstetrics (FIGO). Roman numerals 0, I, II, III, and IV (0 to 4) stand for the different stages of the cancer. The higher the number, the more advanced the cancer is.
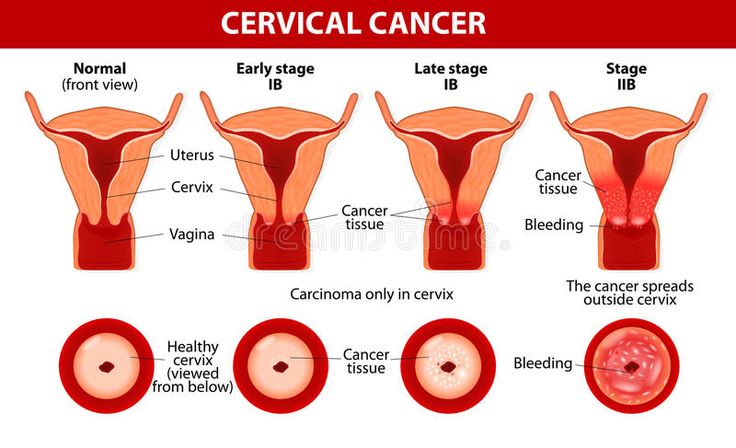
Stage 0
This stage is not part of the FIGO system. Stage 0 is also called carcinoma in situ (CIS). The cancer has grown only in the surface layer of cells lining your cervix. It's not cancer, but a serious precancer. This means that if it's not treated it may turn into true cervical cancer.
Stage I
This cancer has grown deeper into your cervix. It has not spread. Stage I is then divided into these groups:
Stage IA2.
The cancer can only be seen with a microscope. It's between 3 and 5 mm deep.
Stage IB1.
The tumor can be seen without a microscope. It's more than 5 mm deep, but not more than 2 cm in size.
Stage IB2.
The tumor can be seen without a microscope. It's between 2 and 4 cm in size.
Stage IB3.
The tumor can be seen without a microscope. It's at least 4 cm in size.
Stage II
The cancer has spread beyond your cervix and uterus. It has not spread to the walls of your pelvis or to the lower part of your vagina. It has not spread to lymph nodes or distant parts of your body. Stage II is then divided into these groups:
Stage IIA.
The cancer has not spread to the tissues next to the cervix, called the parametria.
Stage IIA1.
The cancer is less than 4 cm in size.
Stage IIA2.
The cancer is more than 4 cm in size.
Stage IIB
This cancer has spread to the tissues around your vagina and cervix (the parametria).
Stage III
The cancer has spread to your lower vagina or to the walls of your pelvis, or it may be causing kidney problems. It might or might not have spread to nearby lymph nodes. It has not spread to distant parts of your body. Stage III is then divided into these groups:
Stage IIIA.
The cancer has spread to the lower part of your vagina. It has not spread to the wall of your pelvis. It has not spread to nearby lymph nodes.
Stage IIIB.
The cancer has spread to the wall of your pelvis. It may block urine flow from your kidneys to your bladder, causing kidney problems (hydronephrosis). It has not spread to nearby lymph nodes.
Stage IIIC1.
The cancer is any size and has spread to nearby pelvic lymph nodes.
Stage IIIC2.
The cancer is any size and has spread to lymph nodes around your aorta.
Stage IV
The cancer has spread to nearby organs, like your bladder, rectum, or to other parts of your body, like your liver or lungs. Stage IV is then divided into these groups:
Stage IVA.
The cancer has spread to nearby organs, like your bladder or rectum, or it's growing outside your pelvis.
Stage IVB.
The cancer has spread to distant organs beyond your pelvis, such as your liver, lungs, bones, or distant lymph nodes.
Treatment Options for Cervical Cancer, by Stage
The stage of a cervical cancer is the most important factor in choosing treatment. But other factors can also affect your treatment options, including the location of the cancer within the cervix, the type of cancer (squamous cell or adenocarcinoma), your age, your overall health, and whether you want to have children.
Stage IA1
Treatment for this stage depends on whether or not you want to be able to have children (maintain fertility) and whether or not the cancer has grown into blood or lymph vessels (called lymphovascular invasion).
Treatment options if you want to maintain fertility
A cone biopsy is the preferred procedure if you want to have children after the cancer is treated.
If the edges of the cone don’t contain cancer cells (called negative margins), the woman can be watched closely without further treatment as long as the cancer doesn’t come back.
If the edges of the cone biopsy have cancer cells (called positive margins), then cancer may have been left behind. This can be treated with a repeat cone biopsy or a radical trachelectomy.
If the cone biopsy shows that the cancer has grown into blood or lymph vessels, it would then be treated the same as stage IA2 disease (see below).
Treatment options if you don’t want to maintain fertility
A simple hysterectomy may be an option if the cancer shows no lymphovascular invasion and the edges of the biopsy have no cancer cells. If the edges of the biopsy have cancer cells present, a repeat cone biopsy or a radical hysterectomy with removal of the pelvic lymph nodes might be an option.
If the cancer has grown into blood or lymph vessels, you might need a radical hysterectomy along with removal of the pelvic lymph nodes. Sometimes, surgery is not done and external beam radiation to the pelvis followed by brachytherapy is used.
If none of the lymph nodes are found to have cancer, radiation may still be discussed as an option if the tumor is large, if the tumor has grown into blood or lymph vessels, or if the tumor is invading the surrounding connective tissue (the stroma) that supports organs such as the uterus, bladder, and vagina.
If the cancer has spread to the tissues next to the uterus (called the parametria) or to any lymph nodes, or if the tissue removed has positive margins, radiation (EBRT) with chemotherapy is usually recommended. The doctor may also advise brachytherapy after the combined chemo and radiation are done.
Stage IA2
Treatment for this stage depends in part on whether or not you want to continue to be able to have children (maintain fertility).
Treatment options if you want to maintain fertility
Cone biopsy with removal of pelvic lymph nodes. (pelvic lymph node dissection)
Radical trachelectomy with pelvic lymph node dissection.
Treatment options if you don’t want to maintain fertility
External beam radiation therapy (EBRT) to the pelvis plus brachytherapy.
Radical hysterectomy with removal of pelvic lymph nodes.
If none of the lymph nodes have cancer cells, radiation may still be an option if the tumor is large, if the tumor has grown into blood or lymph vessels, or if the tumor is invading the surrounding connective tissue (the stroma) that supports organs such as the uterus, bladder, and vagina.
If the cancer has spread to the tissues next to the uterus (called the parametria) or to any lymph nodes, or if the tissue removed has positive margins, radiation (EBRT) with chemotherapy is usually recommended. The doctor may also advise brachytherapy after the combined chemo and radiation are done.
Stages IB and IIA
Stages IB1 and IB2: Treatment options if you want to maintain fertility
Radical hysterectomy with removal of lymph nodes in the pelvis and sometimes lymph nodes from the para-aortic area. If none of the lymph nodes are found to have cancer, radiation may still be discussed as an option if the tumor is large, if the tumor has grown into blood or lymph vessels, or if the tumor is invading the surrounding connective tissue (the stroma) that supports organs such as the uterus, bladder, and vagina. If the cancer has spread to the tissues next to the uterus (called the parametria) or to any lymph nodes, or if the tissue removed has positive margins, radiation (EBRT) with chemotherapy is usually recommended. The doctor may also advise brachytherapy after the combined chemo and radiation are done.
Radiation to the pelvis using both brachytherapy and external beam radiation therapy may be an option if a patient is not healthy enough for surgery or decides they do not want surgery. Chemotherapy (chemo) may be given with the radiation (concurrent chemoradiation).
Stages IB3 and IIA2
Treatment options
Chemoradiation: The chemo may be cisplatin orcarboplatin, given concurrently with external beam radiation (EBRT). , This may be followed by brachytherapy.
Radical hysterectomy with pelvic lymph node dissection and possibly para-aortic lymph node sampling: If cancer cells are found in the removed lymph nodes, or in the edges of the tissue removed (positive margins), surgery may be followed by radiation therapy, which is often given with chemo (concurrent chemoradiation).
Chemoradiation and brachytherapy followed by a hysterectomy. This is not commonly done, but may be an option for certain patients.
Stages IIB, III, IVA
Treatment options
Chemoradiation: The chemo may be cisplatin or carboplatin, given concurrently (at the same time) with external beam radiation (EBRT). This may be followed by brachytherapy.
Stage IVB
At this stage, the cancer has spread outside the pelvis to other areas of the body. Stage IVB cervical cancer is not usually considered curable. Treatment options include chemo alone or with pembrolizumab if the tumor is PD-L1 positive. If chemo is given alone, it's usually a combination of cisplatin or carboplatin with paclitaxel and bevacizumab. If chemo is given with pembrolizumab, chemo is usually cisplatin or carboplatin with paclitaxel, with or without bevacizumab. Radiation therapy may be given to help relieve symptoms. For disease that recurs after initial systemic therapy, other chemo drugs, or immunotherapy alone, or targeted therapy may also be options.
Clinical trials are testing other combinations of chemo drugs, as well as some other experimental treatments.
Recurrent cervical cancer
Cancer that comes back after treatment is called recurrent cancer. Cancer can come back locally (in or near where it first started, such as the cervix, uterus or nearby the pelvic organs), or it can come back in distant areas (such as the lungs or bone).
If the cancer has recurred in the center of the pelvis only, extensive surgery (such as pelvic exenteration) may be an option for some patients, and offers the best chance for possibly curing the cancer (although it can have major side effects). Radiation therapy (sometimes along with chemo) might be another option. If not, chemo, immunotherapy, or targeted therapy may be used to slow the growth of the cancer or help relieve symptoms, but they aren’t expected to cure the cancer.
New treatments that may benefit patients who have distant recurrence of cervical cancer are being evaluated in clinical trials.
No matter which type of treatment your doctor recommends, it's important that you understand the goal of treatment (to try to cure the cancer, control its growth, or relieve symptoms), as well as its possible side effects and limitations. For example, sometimes chemo can improve your quality of life, and other times it might diminish it. You might need to discuss this with your doctor.
New treatments that may benefit patients who have distant recurrence of cervical cancer are being evaluated in clinical trials.
Cervical cancer in pregnancy
A small number of cervical cancers are found in pregnant women. Most of these (70%) are stage I cancers. The treatment plan during pregnancy is determined by:
Tumor size
If nearby lymph nodes
have cancer
have cancer
How far along the pregnancy is
The specific type of cervical cancer
If the cancer is at a very early stage, such as stage IA, most doctors believe it is safe to continue the pregnancy to term and have treatment several weeks after birth. Surgery options after birth for early-stage cancers include a hysterectomy, radical trachelectomy, or a cone biopsy.
If the cancer is stage IB or higher, then you and your doctor must decide whether to continue the pregnancy. If not, treatment would be radical hysterectomy and/or radiation. Sometimes chemotherapy can be given during the pregnancy (in the second or third trimester) to shrink the tumor.
If you decide to continue the pregnancy, the baby should be delivered by cesarean section (C-section) as soon as it is able to survive outside the womb. More advanced cancers typically need be treated immediately.